Torsades de Pointes (Polymorphic VT) — ECG Rhythm | Telemetric Pro
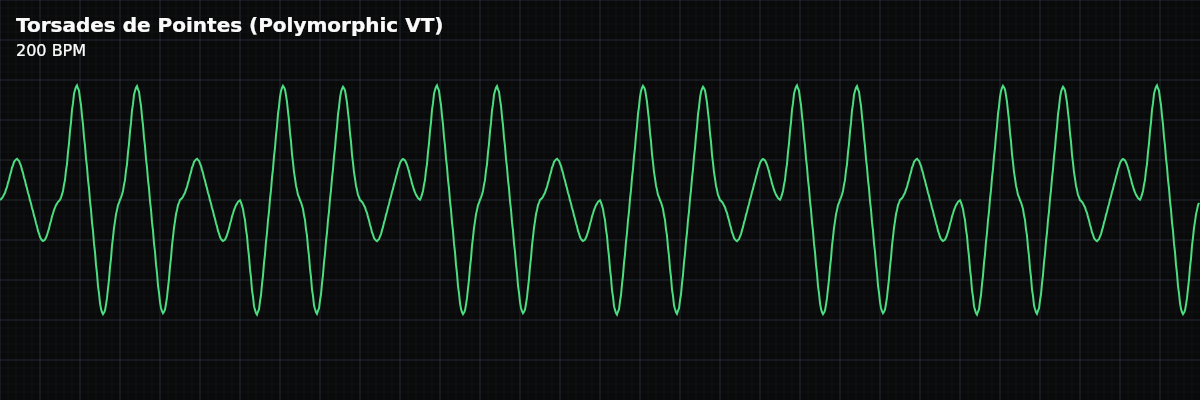
A distinctive polymorphic ventricular tachycardia where the QRS complexes appear to twist around the baseline — amplitude waxes and wanes as polarity gradually shifts. Associated with prolonged QT interval.
| Rate | 150–300 bpm |
|---|---|
| Rhythm | Irregular (continuously changing) |
| P Waves | Absent |
| PR Interval | Not applicable |
| QRS Duration | Wide, polymorphic (“twisting” pattern) |
Torsades de Pointes — French for "twisting of the points" — is one of the most visually distinctive rhythms in ECG interpretation. The QRS complexes appear to spin around the baseline: the amplitude gradually increases, reaches a peak, then decreases and reverses polarity, creating a sinusoidal waxing-and-waning pattern. This is not random chaos like VFib — it has an organized, almost hypnotic pattern.
For monitor technicians, recognizing Torsades is critical because its treatment is fundamentally different from standard VT. The usual VT drugs (amiodarone, procainamide, sotalol) prolong the QT interval — exactly the wrong thing to do in Torsades, where QT prolongation is the underlying problem. Recognizing the twisting pattern and communicating "this looks like Torsades" helps the clinical team choose the right treatment.
What Changed from Normal Sinus Rhythm
Torsades replaces normal rhythm with a rapid, wide-complex tachycardia where the QRS morphology continuously changes. No P waves are visible. The rate is extremely fast (150-300 BPM). What makes it unique is the organized waxing-and-waning amplitude pattern — the QRS "twists" around the baseline rather than being randomly chaotic.
Five Criteria: Torsades de Pointes
- Rate: 150-300 BPM
- Extremely rapid. The rate may vary during the episode. Hemodynamically significant — patients are usually symptomatic or unconscious.
- Regularity: Irregular (continuously changing)
- The rhythm is irregular because the QRS morphology and amplitude are continuously changing. No two consecutive beats look identical.
- P Waves: Absent
- P waves cannot be identified in the rapid, chaotic ventricular waveform. The rhythm is entirely ventricular in origin.
- QRS: Wide, polymorphic — "twisting" pattern
- The QRS amplitude waxes and wanes over 5-20 beats. Polarity gradually shifts from positive to negative and back. This creates the characteristic spindle-shaped envelope that distinguishes Torsades from VFib.
- Baseline QT: Prolonged (> 500ms)
- Check the QTc on beats before and after the episode. A prolonged QT strongly supports the diagnosis of Torsades (vs generic polymorphic VT from ischemia).
What Torsades Looks Like on the Strip
On the monitor, Torsades is unmistakable once you have seen it: a rapid, wide-complex tachycardia where the QRS complexes appear to rotate around the baseline in a smooth, organized pattern. The amplitude gradually grows, reaches a peak, then shrinks and reverses — like a spinning top viewed from the side. This distinguishes it from VFib (random chaos) and monomorphic VT (uniform morphology).
Why Torsades Treatment Differs from Standard VT
This is the critical clinical distinction: **Standard (Monomorphic) VT** — Treat with amiodarone, procainamide, or lidocaine. These drugs work for re-entrant circuits in structurally abnormal hearts. **Torsades de Pointes** — These same drugs can WORSEN Torsades because they prolong the QT interval further. The correct approach is to shorten the QT: IV magnesium (first-line), correct electrolytes, increase the heart rate (overdrive pacing or isoproterenol), and stop all QT-prolonging drugs.
Clinical Context for Monitor Technicians
Common triggers for Torsades include: QT-prolonging drugs (sotalol, amiodarone, antipsychotics, certain antibiotics, methadone), electrolyte abnormalities (hypokalemia, hypomagnesemia, hypocalcemia), congenital long QT syndrome, bradycardia (which further prolongs the QT), and hypothermia. The classic initiation sequence is "short-long-short": a PVC, a compensatory pause (which prolongs the QT even more), then another PVC landing on the vulnerable period, triggering the arrhythmia.
When to Escalate
**Notify immediately:** - Any episode of Torsades (twisting polymorphic VT) - Patient is unresponsive or pulseless (defibrillation needed) - Recurrent episodes (QT must be corrected to prevent recurrence) - Prolonged QT (> 500ms) with any ventricular ectopy (precursor to Torsades) Torsades is never a "document and monitor" rhythm. It always requires immediate notification.
Putting It Together
Torsades de Pointes is a polymorphic VT at 150-300 BPM with a characteristic twisting pattern — QRS amplitude waxes and wanes as polarity shifts around the baseline. Associated with prolonged QT. Treatment differs critically from standard VT: IV magnesium (not amiodarone), correct electrolytes, increase heart rate, stop QT-prolonging drugs. Recognizing the pattern and communicating "Torsades" helps guide correct treatment.