Third Degree AV Block (Complete Heart Block) — ECG Rhythm | Telemetric Pro
Complete failure of AV conduction — no atrial impulses reach the ventricles. The atria and ventricles beat independently (AV dissociation), and the ventricles are sustained only by an escape rhythm.
| Rate | Ventricular 20–60 bpm (escape dependent) |
|---|---|
| Rhythm | Regular (P and QRS each regular, independent) |
| P Waves | Present, march through independently of QRS |
| PR Interval | Variable (no relationship to QRS) |
| QRS Duration | Narrow or wide (depends on escape level) |
Third Degree AV Block — Complete Heart Block — is the end of the AV block spectrum. In first degree, all beats conduct slowly. In second degree, some beats are dropped. In third degree, nothing gets through. The AV node (or infranodal conduction system) has completely failed, and the atria and ventricles beat as two entirely independent units.
For monitor technicians, complete heart block is one of the most recognizable critical rhythms. You see two independent rhythms running simultaneously: P waves marching at one rate and QRS complexes marching at a slower rate, with no relationship between them. The patient depends entirely on the escape rhythm — which is slow and potentially unreliable.
What Changed from Normal Sinus Rhythm
Complete heart block changes everything from NSR: the pacemaker relationship is broken (atria and ventricles are independent), the ventricular rate is slow (escape rhythm), the PR interval is meaningless (varies randomly), and the QRS may be wide (if ventricular escape). The P waves themselves are still normal — the SA node is working fine. The problem is that its impulses cannot reach the ventricles.
Five Criteria: Complete Heart Block vs NSR
- Rate: Slow (depends on escape focus)
- Atrial rate is normal (60-100 BPM). Ventricular rate depends on the escape: junctional escape (40-60) or ventricular escape (20-40). The atrial and ventricular rates are always different.
- Regularity: Regular (both independently)
- Both P-P intervals and R-R intervals are individually regular. But they are at different rates. This "two independent regular rhythms" is the signature of complete heart block.
- P Waves: Present, normal — but independent of QRS
- P waves march at their own rate, completely unrelated to the QRS complexes. P waves may appear before, during, or after QRS complexes — their position shifts from beat to beat as the two rhythms drift in and out of alignment.
- PR Interval: Variable (no relationship)
- The PR interval changes randomly from beat to beat because there is no conduction between atria and ventricles. The varying PR is diagnostic — in second degree blocks, conducted beats have a consistent PR.
- QRS Complex: Depends on escape focus
- Narrow QRS = junctional escape (block at AV node, escape from junction, 40-60 BPM, better prognosis). Wide QRS = ventricular escape (block infranodal, escape from Purkinje, 20-40 BPM, worse prognosis).
What Complete Heart Block Looks Like on the Strip
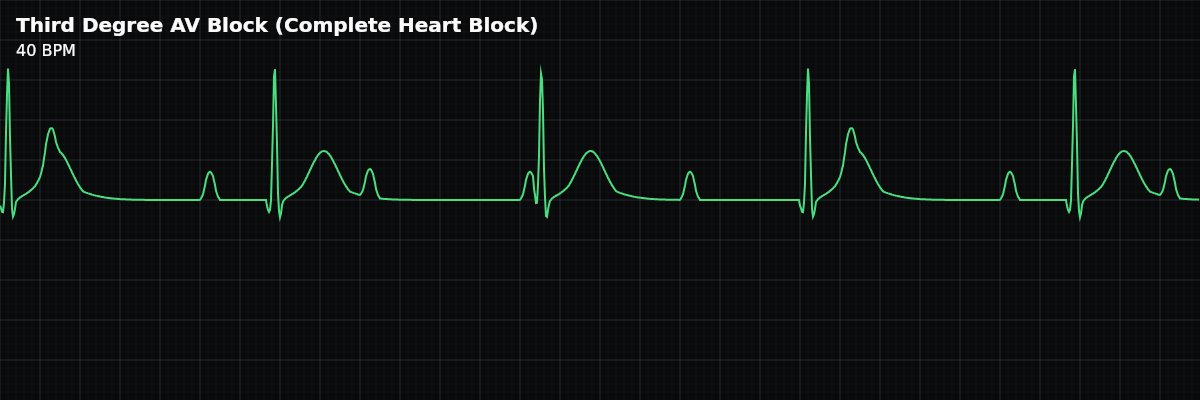
On the strip, complete heart block is unmistakable once you see it: P waves marching at one rate and QRS complexes marching at a different, slower rate. The P waves appear to "walk through" the QRS complexes — sometimes falling before, sometimes during, sometimes after the QRS. Use calipers: set them to the P-P interval and confirm the P waves are regular. Then set them to the R-R interval and confirm the QRS complexes are regular. If both are regular but at different rates, you have complete heart block.
The Complete AV Block Spectrum
Third degree block is the end of a progression: **First Degree** — All beats conduct, but slowly (PR > 200ms). A delay. **Second Degree Type I** — PR progressively lengthens until a beat drops. A pattern. **Second Degree Type II** — Beats drop suddenly without PR change. A warning. **Second Degree 2:1** — Every other beat drops. Ambiguous type. **Third Degree** — No beats conduct at all. Complete dissociation. Understanding this progression helps you recognize when a patient is worsening. If second degree block progresses to third degree, the clinical urgency escalates dramatically.
Going Deeper: AV Dissociation Is Not Always AV Block
Locating the Block: The 4-Step Algorithm
Clinical Context for Monitor Technicians
Complete heart block is most commonly seen with acute MI (inferior MI usually produces AV nodal block that may resolve; anterior MI produces infranodal block that often requires permanent pacing), degenerative conduction disease, drug toxicity (beta-blockers, calcium channel blockers, digoxin), post-cardiac surgery, myocarditis (including Lyme disease), and infiltrative diseases.
When to Escalate
**Notify immediately:** - Any complete heart block — this always requires urgent evaluation - Wide QRS escape rhythm (ventricular escape at 20-40 BPM — less reliable) - Patient is symptomatic — syncope, altered consciousness, hypotension - Escape rate is dropping or becoming irregular (escape failure imminent) - New complete heart block in an acute MI patient Complete heart block is never a "document and monitor" rhythm. It always requires immediate notification.
Transcutaneous Pacing on the Monitor
When transcutaneous pacing is initiated for complete heart block, the monitor shows tall, wide pacing spikes followed by wide QRS complexes — this confirms mechanical capture. The spikes are much larger than permanent pacemaker spikes because the energy is delivered through skin electrodes on the chest wall rather than through a wire directly on the heart muscle. Spikes without QRS = no capture. Spikes with wide QRS = capture. If you see intermittent capture (some spikes produce QRS complexes, others do not), report it — the output may need adjustment.