Second Degree AV Block Type I (Wenckebach) — ECG Rhythm | Telemetric Pro
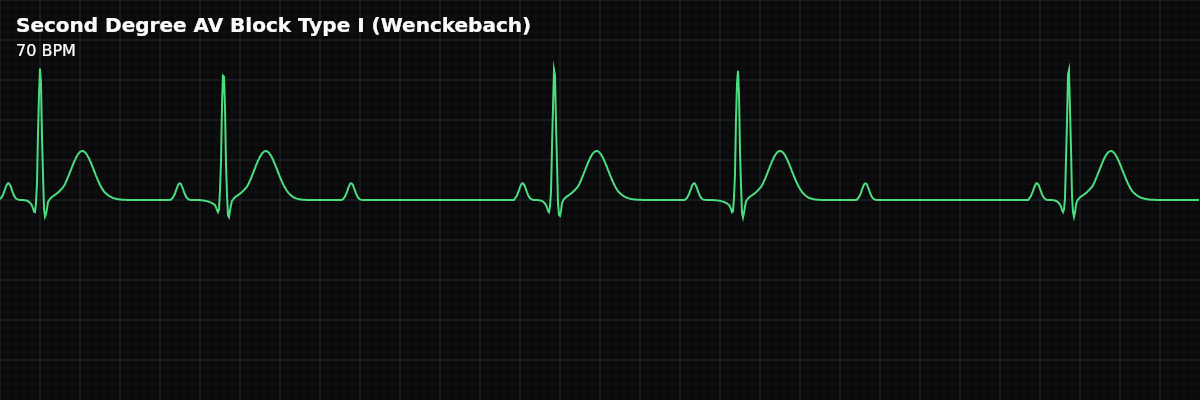
Progressive PR interval prolongation with each successive beat until one P wave fails to conduct, producing a dropped QRS. The cycle then repeats, creating a characteristic "group beating" pattern.
| Rate | Variable (atrial > ventricular) |
|---|---|
| Rhythm | Irregular (grouped beating pattern) |
| P Waves | Upright, more P waves than QRS complexes |
| PR Interval | Progressively prolonging until dropped QRS |
| QRS Duration | < 0.12 s |
Second Degree AV Block Type I — the Wenckebach phenomenon — is one of the most elegant patterns in ECG interpretation. The AV node is becoming progressively more fatigued with each successive beat: the first impulse gets through easily, the second with more delay, the third with even more delay, until finally one impulse is completely blocked. Then the AV node rests during the pause, recovers, and the cycle starts over.
For monitor technicians, Wenckebach is recognizable by its distinctive "group beating" pattern — clusters of beats separated by pauses that repeat in a predictable cycle. Once you learn to spot this pattern on the monitor, you can identify Wenckebach at a glance even before measuring PR intervals.
What Changed from Normal Sinus Rhythm
Wenckebach changes two things from NSR: the PR interval (progressively lengthens instead of staying constant) and the regularity (group beating with pauses instead of regular rhythm). The P waves remain normal and regular — the SA node fires on schedule throughout. The QRS is narrow because the block is at the AV node, above the bundle branches.
Five Criteria: Wenckebach vs NSR
- Rate: Variable
- Atrial rate is regular (SA node fires normally). Ventricular rate is slower because some beats are dropped. The effective ventricular rate depends on the conduction ratio (3:2, 4:3, 5:4).
- Regularity: Irregularly irregular (group beating)
- Clusters of conducted beats are separated by pauses (dropped beats). The pattern is predictable: beats get progressively closer together, then a pause occurs. This creates the "group beating" pattern.
- P Waves: Normal, regular — more P waves than QRS complexes
- P waves march out at a constant rate. Every P wave looks the same. But some P waves are not followed by a QRS — these are the dropped beats. Count the P waves and QRS complexes: you will find more P waves.
- PR Interval: Progressively lengthens then resets
- The first PR after a dropped beat is the shortest. Each subsequent PR gets longer. The longest PR occurs just before the dropped beat. After the pause, the PR resets to its shortest value.
- QRS Complex: Narrow (<0.12s)
- The block is at the AV node level, above the bundle branches. Ventricular conduction is normal for all conducted beats. A narrow QRS supports the diagnosis of Type I (AV nodal) rather than Type II (infranodal).
What Wenckebach Looks Like on the Strip
On the monitor, the group beating pattern is the first thing you notice: beats come in clusters with pauses between them. Within each cluster, the beats appear to get progressively closer together (because the PR increment decreases with each beat). Then a pause occurs (the dropped beat), and the cycle starts over. On a strip, you can confirm by measuring PR intervals: each gets longer until one P wave stands alone without a QRS.
Type I (Wenckebach) vs Type II (Mobitz II)
This is one of the most critical distinctions in AV block interpretation: **Type I (Wenckebach)** — PR progressively lengthens before the dropped beat. Block is at the AV node. QRS is usually narrow. Generally benign and often reversible. Rarely requires pacing. **Type II (Mobitz II)** — PR is constant before the dropped beat. Block is below the AV node (infranodal). QRS is often wide. More dangerous — can progress suddenly to complete heart block. Often requires pacing.
Marriott's "Footprints" of Wenckebach
The classic teaching focuses on PR intervals, but Marriott emphasized the **RR interval pattern** — which is what you actually see at a glance on the monitor before measuring anything. He called these three features the "footprints" of Wenckebach:
These footprints are powerful because you can spot them on the monitor before pulling a strip: clusters of beats that get progressively closer together, then a pause, then the pattern repeats. As Marriott wrote: **"Decremental conduction delay may occur in any cardiac conduction pathway. Group beating is the hallmark of such activity."**
When Wenckebach Doesn't Follow the Textbook
The classic Wenckebach pattern — steadily increasing PR intervals with the biggest jump between the first and second beats — is actually the exception rather than the rule. Both the sinus rate and AV conduction are under constant autonomic influence, which distorts the textbook pattern. Marriott identified four common variants:
Going Deeper: Why the PR Varies
Clinical Context for Monitor Technicians
Wenckebach is generally considered benign and often reversible. Common causes include increased vagal tone (athletes, sleep), medications (beta-blockers, calcium channel blockers, digoxin), inferior MI affecting the AV node, myocarditis, and post-cardiac procedures. In athletes and young individuals, it may be a normal finding during rest or sleep.