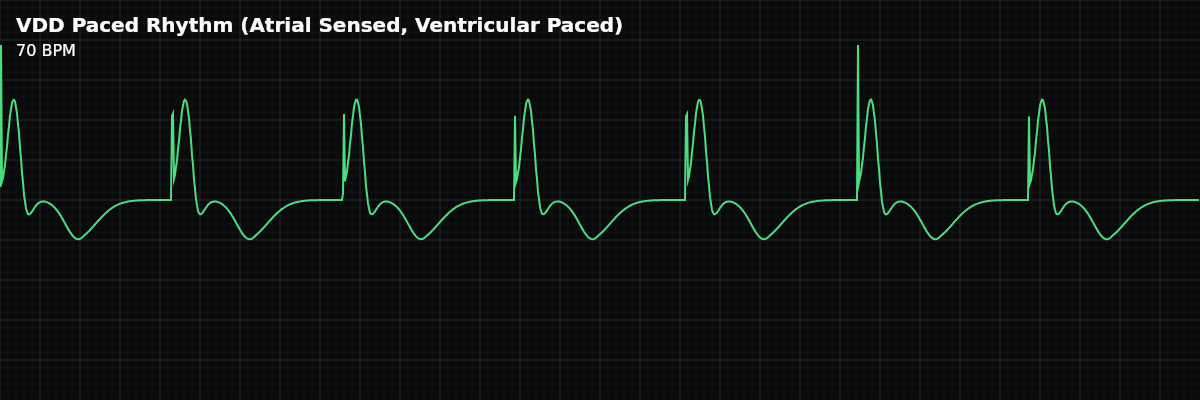
VDD Paced Rhythm (Atrial Sensed, Ventricular Paced) — ECG Rhythm | Telemetric Pro
A pacing mode that senses native atrial activity and paces the ventricle after a programmed AV delay. Maintains AV synchrony using the patient's own SA node — no atrial spike on the strip.
| Rate | Tracks native sinus rate (60–130 bpm) |
|---|---|
| Rhythm | Regular |
| P Waves | Native sinus P waves (sensed, not paced) |
| PR Interval | Programmed AV delay (120–200 ms) |
| QRS Duration | > 0.12 s (wide, paced morphology) |
VDD pacing is a clever single-lead solution for patients who need ventricular pacing but have a healthy SA node. The pacemaker senses the native P wave, waits for a programmed AV delay, then paces the ventricle. This preserves AV synchrony — the ventricles contract in coordination with the atria — while requiring only a single lead with floating atrial electrodes (electrodes positioned along the atrial segment of the lead body — not actively fixed like standard leads, but passively resting in the bloodstream to sense atrial activity).
For monitor technicians, VDD pacing has a distinctive appearance: native P waves (no atrial spike) followed by a ventricular spike and wide QRS. The heart rate varies naturally with the patient's sinus rate — faster with activity, slower at rest — because the pacemaker is tracking the patient's own SA node. This distinguishes it from fixed-rate ventricular pacing.
What Changed from Normal Sinus Rhythm
VDD pacing changes the ventricular activation (paced wide QRS instead of normal narrow QRS) while preserving normal atrial timing. The P waves are native and normal — the SA node is working. The key difference from NSR is below the AV node: the impulse is blocked (AV block), and the pacemaker substitutes for the failed conduction.
Five Criteria: VDD Paced vs NSR
- Rate: Tracks native sinus rate
- The ventricular rate follows the patient's sinus rate. During exercise, the rate increases naturally because the pacemaker tracks faster P waves. This provides physiologic rate response without rate-responsive sensors.
- Regularity: Regular
- The rhythm is regular because the pacemaker tracks each native P wave with a fixed AV delay. The regularity reflects the underlying sinus rhythm.
- P Waves: Native (no atrial spike)
- Normal sinus P waves are present — the SA node fires naturally. There is NO pacing spike before the P wave. This is the key distinction from DDD pacing.
- PR Interval: Programmed AV delay (sensed P to V spike)
- The interval from the native P wave to the ventricular spike is the programmed sensed AV delay. It is constant and replaces the normal AV conduction.
- QRS Complex: Wide (>0.12s) — ventricular pacing
- The ventricular pacing electrode produces a wide QRS with LBBB morphology — identical to VVI pacing. The wide QRS occurs because depolarization spreads from the electrode, not through the His-Purkinje system.
What VDD Pacing Looks Like on the Strip
On the strip, VDD pacing shows a distinctive pattern: native P waves (no atrial spike) followed by a ventricular spike and wide QRS. The heart rate varies with the patient's sinus rate — you will see it change naturally with activity and rest. The interval from P wave to ventricular spike is constant (the programmed AV delay).
VDD vs DDD Pacing
The critical distinction between VDD and DDD: **VDD** — Senses the atrium, paces the ventricle. Native P waves (no atrial spike). Cannot pace the atrium. Requires intact SA node. **DDD** — Can pace AND sense both chambers. May have atrial spikes before P waves. Can pace the atrium if the SA node fails. More versatile but requires two leads. On the strip: native P waves + V spike only = VDD. Atrial spike + P wave + V spike = DDD.
Clinical Context for Monitor Technicians
VDD pacing is used specifically for high-grade AV block with normal sinus node function. The patient's SA node provides rate response, and the pacemaker substitutes for the failed AV conduction. VDD has become less common as DDD systems have improved, but it remains valid when minimizing leads is important or when the patient has proven reliable sinus function.
When to Escalate
**Notify promptly:** - Sudden drop to fixed lower rate (loss of atrial tracking) - Ventricular spikes without QRS (failure to capture) - Loss of AV synchrony (P waves and spikes become unrelated) - Patient becomes symptomatic — dizziness, exercise intolerance, fatigue **Document and monitor:** - Stable VDD pacing with consistent P-to-spike intervals and rate that varies with activity - Normal functioning: rate increases with exercise and slows at rest
What Happens When...
**Patient exercises** — The pacing rate increases, and that is normal. VDD pacing tracks the native sinus rate, so when the patient becomes more active, the SA node fires faster and the pacemaker follows. You will see the same P-wave-to-V-spike relationship at the faster rate — the AV delay remains constant. Unlike VVIR, which uses sensors to estimate activity, VDD provides truly physiologic rate response because it follows the patient's own SA node.