Ventricular Paced Rhythm (VVI) — ECG Rhythm | Telemetric Pro
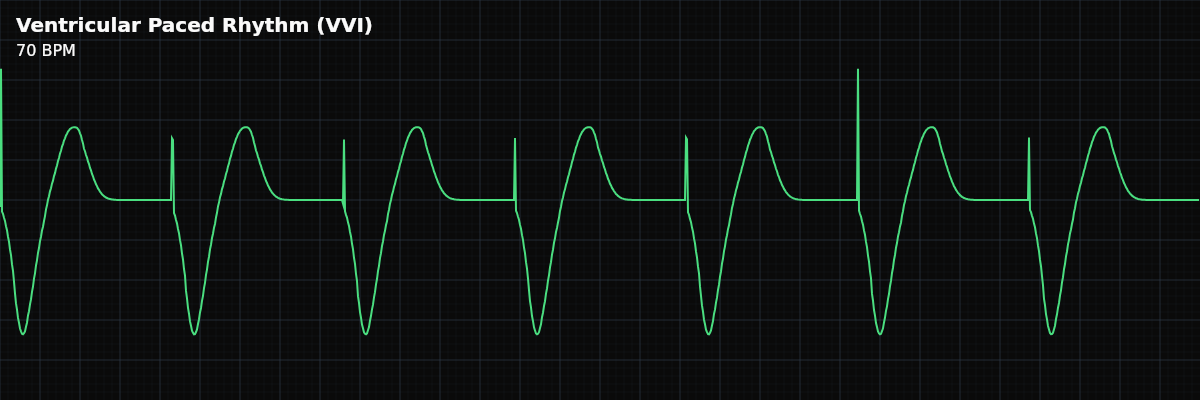
A pacemaker directly stimulates the ventricles, producing a wide QRS with LBBB morphology. The most recognizable paced rhythm — a spike immediately before each wide QRS complex.
| Rate | 60–70 bpm (programmed) |
|---|---|
| Rhythm | Regular |
| P Waves | May be absent or dissociated |
| PR Interval | Not applicable |
| QRS Duration | > 0.12 s (wide, paced morphology) |
Ventricular pacing is the workhorse of cardiac pacing — and the most recognizable paced rhythm on the monitor. The pacemaker directly stimulates the right ventricle, producing a wide QRS that looks like left bundle branch block. The wide QRS occurs because the impulse spreads from the pacing electrode through the ventricular myocardium rather than through the rapid His-Purkinje conduction system.
For monitor technicians, VVI pacing is a rhythm you will see frequently. The pattern is distinctive: a sharp spike followed immediately by a wide QRS. Your critical skills are confirming capture (every spike produces a QRS), checking for appropriate sensing (the pacemaker inhibits when native beats occur), and recognizing malfunctions.
What Changed from Normal Sinus Rhythm
VVI pacing changes the pacemaker source (ventricle instead of SA node) and the QRS (wide instead of narrow). P waves may be absent or dissociated — the pacemaker does not sense or pace the atria, so native atrial activity (if any) occurs independently. This loss of AV synchrony is the main hemodynamic limitation of VVI pacing.
Five Criteria: VVI Paced vs NSR
- Rate: Set by pacemaker (typically 60-70 BPM)
- The lower rate limit is programmed. The pacemaker fires at this rate whenever the native ventricular rate drops below it. Some VVI pacemakers have rate-responsive features that increase the rate during physical activity.
- Regularity: Regular
- The paced rhythm is regular at the programmed rate. If native beats occur faster than the paced rate, the pacemaker inhibits and you see native beats interspersed with paced beats.
- P Waves: Independent or absent
- VVI does not sense or pace the atria. If the SA node is working, P waves may march at their own rate (AV dissociation). If the SA node is also dysfunctional, P waves may be absent.
- PR Interval: Not applicable
- There is no conduction relationship between atria and ventricles. If P waves are present, their timing relative to the QRS is random — like complete heart block.
- QRS Complex: Wide (>0.12s) with LBBB morphology
- The pacing electrode in the RV apex depolarizes the ventricles from right to left. QRS is typically >140ms with LBBB pattern. Every paced QRS looks the same (monomorphic).
What VVI Pacing Looks Like on the Strip
On the monitor, VVI pacing is instantly recognizable: regular, wide QRS complexes at a steady rate, each preceded by a sharp spike. The wide QRS has a consistent morphology (every paced beat looks the same). Look for independent P waves — small bumps that march at their own rate, unrelated to the paced QRS complexes.
Clinical Context for Monitor Technicians
VVI pacing is most commonly used in patients with permanent atrial fibrillation and slow ventricular response (since AV synchrony is impossible anyway). It is also used as a backup pacing mode in ICDs and for patients with limited life expectancy where a simpler system is appropriate. For most other indications, VVI has been largely replaced by dual-chamber (DDD) pacing to maintain AV synchrony.
When to Escalate
**Notify promptly:** - Spikes without QRS complexes (failure to capture) - Native beats not inhibiting the pacemaker (failure to sense — oversensing or undersensing) - Paced rate significantly different from programmed rate - Patient becomes symptomatic — dizziness, fatigue, neck pulsations (pacemaker syndrome) - Sudden loss of all pacing output **Document and monitor:** - Stable VVI pacing with consistent capture and appropriate sensing - Occasional native beats interspersed (normal pacemaker behavior)
What Happens When...
**Patient exercises** — In rate-responsive mode (VVIR), the pacemaker uses an accelerometer or minute ventilation sensor to detect activity and increase the ventricular pacing rate. On the monitor, you will see the paced rate climb gradually during activity and return to the programmed lower rate limit at rest. The QRS remains wide throughout — the morphology does not change, only the rate. This is expected behavior, not a malfunction.
**Atrial fibrillation** — VVI is often the pacing mode chosen for patients with permanent atrial fibrillation, because AV synchrony is already impossible in AFib. If AFib is already present, VVI continues to function normally — it paces the ventricle regardless of atrial activity. If NEW AFib develops in a patient who was previously in sinus rhythm, the pacing pattern itself does not change, but the overall rhythm may become irregular between paced beats as native conducted beats from the AFib compete with the pacemaker. The independent P waves you may have seen before will be replaced by a fibrillatory baseline. Report the rhythm change.