Second Degree AV Block Type II (Mobitz II) — ECG Rhythm | Telemetric Pro
Intermittent failure of AV conduction where beats drop suddenly without PR prolongation. The block is infranodal and carries a high risk of progression to complete heart block.
| Rate | Variable (atrial > ventricular) |
|---|---|
| Rhythm | Irregular (sudden dropped QRS) |
| P Waves | Upright, more P waves than QRS complexes |
| PR Interval | Constant on conducted beats |
| QRS Duration | Often wide (> 0.12 s) |
Second Degree AV Block Type II — Mobitz II — is the dangerous sibling in the second degree family. Where Wenckebach gives warning (progressive PR lengthening), Mobitz II drops beats without any warning at all. The PR interval is completely normal one beat, and the next P wave simply fails to conduct. This unpredictability is what makes it dangerous.
For monitor technicians, Mobitz II is a rhythm that demands immediate attention. The block is below the AV node (infranodal), which means the escape rhythm — if one develops when higher-degree block occurs — will be ventricular, slow, and potentially unreliable. Recognizing the constant PR with sudden drops is the key skill.
What Changed from Normal Sinus Rhythm
Mobitz II changes two things from NSR: beats are dropped (some P waves lack a QRS), and the QRS is often wide (because the block is at the bundle branch level). The PR interval — for beats that do conduct — remains constant. The P waves remain normal and regular. The SA node is firing on schedule; only the infranodal conduction fails intermittently.
Five Criteria: Mobitz II vs NSR
- Rate: Variable (often bradycardic)
- Atrial rate is regular (SA node fires normally). Ventricular rate is slower because some beats are dropped. Effective rate depends on the conduction ratio (2:1, 3:1, 4:1).
- Regularity: Irregular (dropped beats without warning)
- The rhythm is interrupted by sudden pauses when P waves fail to conduct. Unlike Wenckebach, there is no predictable group beating pattern — drops can occur at variable intervals.
- P Waves: Normal, regular — more P waves than QRS complexes
- P waves march out at a constant rate. Every P wave looks the same. Some P waves stand alone without a following QRS — these are the dropped beats.
- PR Interval: Constant for all conducted beats
- The PR interval does NOT change before the drop. It may be normal or slightly prolonged, but it is the same from conducted beat to conducted beat. This is the key distinction from Type I.
- QRS Complex: Often wide (>0.12s)
- A wide QRS strongly supports Mobitz II because it localizes the block to the bundle branches. A narrow QRS Mobitz II is rare and may actually be atypical Type I — always correlate clinically.
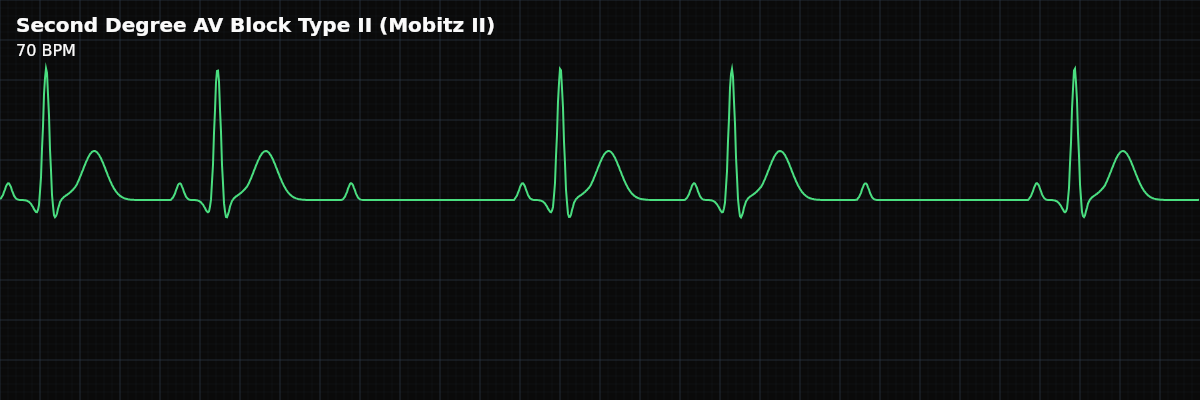
What Mobitz II Looks Like on the Strip
On the strip, Mobitz II looks like a regular rhythm with occasional unexpected pauses. The conducted beats have identical PR intervals — measure them and confirm they do not change. Then you see a P wave standing alone, not followed by a QRS. The rhythm resumes with the same PR interval. No group beating, no progressive lengthening — just a sudden, unexplained drop.
Type II (Mobitz II) vs Type I (Wenckebach)
This is one of the most critical distinctions in rhythm interpretation: **Type I (Wenckebach)** — PR progressively lengthens before the dropped beat. Block is at the AV node. QRS is usually narrow. Generally benign. Group beating pattern. **Type II (Mobitz II)** — PR is constant before the dropped beat. Block is infranodal. QRS is often wide. Dangerous — high risk of sudden complete block. No warning pattern.
Going Deeper: Why Mobitz II Has a Wide QRS
Clinical Context for Monitor Technicians
Mobitz II is uncommon without underlying heart disease. It is most often seen with anterior MI (LAD territory ischemia affecting the bundle branches), degenerative conduction system disease (Lenegre-Lev disease), post-cardiac surgery, myocarditis, and infiltrative diseases (sarcoidosis, amyloidosis). Unlike Wenckebach, it is rarely caused by medications or increased vagal tone.
When to Escalate
**Notify immediately:** - Any new Mobitz II pattern — this rhythm always requires urgent evaluation - Wide QRS with dropped beats (strongly suggests infranodal block) - Increasing frequency of dropped beats (progression toward higher-degree block) - Patient is symptomatic — syncope, near-syncope, hypotension, altered consciousness - Rate dropping below 50 BPM due to frequent dropped beats Mobitz II is never a "document and monitor" rhythm. It always requires prompt notification and evaluation for pacing.
Putting It Together
Mobitz II (Type II second degree AV block) drops beats suddenly without PR prolongation. The PR interval is constant for all conducted beats, and the QRS is often wide because the block is infranodal. This is a dangerous rhythm with a high risk of progression to complete heart block. Distinguish from Type I by the constant PR (Type II) vs progressive PR lengthening (Type I). Always escalate promptly.