Atrio-Ventricular Paced Rhythm (AV Sequential) — ECG Rhythm | Telemetric Pro
A rhythm where an artificial pacemaker stimulates both the atria and the ventricles in sequence, maintaining AV synchrony.
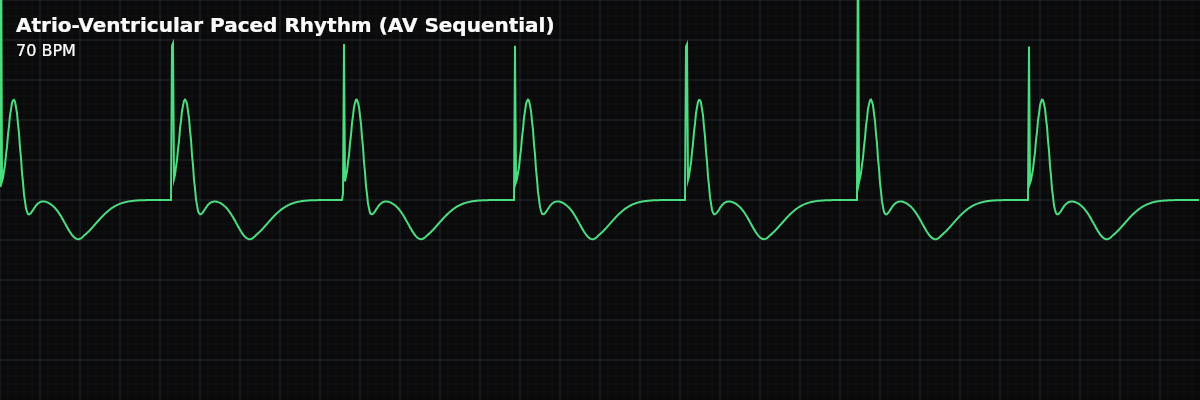
| Rate | 60–80 bpm (programmed) |
|---|---|
| Rhythm | Regular |
| P Waves | Pacing spike before each P wave |
| PR Interval | Programmed AV delay (120–200 ms) |
| QRS Duration | > 0.12 s (wide, paced morphology) |
Every rhythm you have studied so far is generated by the heart itself — the SA node fires, the impulse travels through the conduction system, and the chambers contract. AV Paced Rhythm is fundamentally different: an implanted electronic device is driving the heart. The pacemaker delivers timed electrical impulses to the atria and ventricles, producing a rhythm that looks different from anything the heart generates on its own.
Pacemakers are increasingly common on monitored units. Recognizing a paced rhythm — and knowing what normal pacemaker function looks like — is essential because it changes how you interpret the strip. A wide QRS that would be alarming in a native rhythm is perfectly expected in a paced one. A spike without a following waveform, on the other hand, is a problem that needs immediate attention.
What Changed from Normal Sinus Rhythm
AV paced rhythm introduces features not seen in any native rhythm: pacing spikes before the waveforms, a wide QRS (because the impulse bypasses the normal conduction system), and electronic-precision regularity. The underlying principle is the same as NSR — atria contract, then ventricles contract — but the driver is a machine, not the SA node.
Five Criteria: AV Paced vs Normal Sinus Rhythm
- Rate: Programmed, typically 60-80 bpm (NSR: 60-100)
- The rate is set by the pacemaker and does not change unless the device has rate-responsive features (which adjust for activity). On the monitor, you will see a fixed rate that matches the programmed base rate.
- Regularity: Perfectly regular (NSR: regular with slight variability)
- Paced rhythms are metronomically regular — even more precise than NSR. The electronic timer produces identical R-R intervals down to the millisecond.
- P Waves: Present but paced (NSR: intrinsic, upright)
- A P wave follows each atrial spike, confirming atrial capture. The P wave shape may differ from the patient's native P wave because depolarization starts at the pacing lead, not the SA node.
- PR/AV Delay: 120-200ms (NSR: 120-200ms)
- The AV delay is measured spike-to-spike (not wave-to-wave). It falls in the same range as a native PR interval and serves the same purpose.
- QRS Width: Wide, >120ms (NSR: narrow, <120ms)
- This is the most important difference. The QRS is wide because the ventricular impulse starts at the pacing lead and spreads through muscle tissue rather than the fast His-Purkinje fibers. This is expected and normal.
Rate
The rate in a paced rhythm is determined by the device, not the heart. Most pacemakers are programmed to a base rate of 60-80 bpm. This rate will appear on the monitor as a steady number that does not fluctuate with breathing, position changes, or mild activity — a clue that the rhythm is paced.
The Two Spikes
The two spikes are the signature of AV pacing. The first spike — the **atrial spike** — fires and triggers atrial contraction. After the programmed AV delay, the second spike — the **ventricular spike** — fires and triggers ventricular contraction. This two-spike-per-cycle pattern is what distinguishes AV pacing from single-chamber pacing (which has only one spike).
QRS Complex
The wide QRS is the feature that surprises new learners most. In every rhythm you have studied before, a wide QRS raises concern — it can indicate ventricular origin or conduction disease. In a paced rhythm, the wide QRS is completely expected. The reason is simple: the pacing lead sits in the ventricle, not in the His bundle. When the ventricular spike fires, the impulse spreads through muscle tissue rather than the fast conduction fibers. This slower, muscle-to-muscle conduction takes longer, producing a QRS wider than 120ms — typically 140-200ms.
AV Delay
The AV delay is the time between the atrial spike and the ventricular spike. It serves the same purpose as the PR interval: giving the atria time to finish contracting and fill the ventricles before ventricular contraction begins. Typical values are 120-200ms. Unlike a native PR interval, the AV delay is measured spike-to-spike — the sharp, distinct spikes make measurement straightforward.
Recognizing Pacemaker Malfunction
Normal pacemaker function means: every spike produces a response, and the rhythm runs at the programmed rate. The three malfunctions you need to recognize on the monitor are straightforward:
**Failure to capture** — You see a spike, but no waveform follows. The pacemaker fired, but the heart did not respond. On the strip: a ventricular spike with no QRS, or an atrial spike with no P wave. **Failure to sense** — The pacemaker does not detect the heart's own beats, so it fires when it should not. On the strip: pacing spikes falling in odd locations, sometimes landing on native beats or during the T wave. **Failure to pace** — No spike appears when one is expected. The pacemaker should fire after its programmed interval, but nothing happens. On the strip: a pause longer than the programmed rate with no pacing spike.