Idioventricular Rhythm (IVR) — ECG Rhythm | Telemetric Pro
The heart's last-resort escape rhythm — ventricular pacemaker cells fire at their inherent rate of 20-40 BPM when both the SA node and AV junction have failed.
| Rate | 20–40 bpm |
|---|---|
| Rhythm | Regular |
| P Waves | Absent |
| PR Interval | Not applicable |
| QRS Duration | > 0.12 s (wide) |
Idioventricular Rhythm is the last line of defense. The heart has three levels of pacemaker cells: the SA node (60-100 BPM), the AV junction (40-60 BPM), and the ventricles (20-40 BPM). IVR means both the SA node and AV junction have failed, and the only thing keeping the heart beating is the ventricular Purkinje fibers firing at their slowest inherent rate.
For monitor technicians, IVR is a critical rhythm that demands immediate attention. A rate of 20-40 BPM is barely enough to maintain consciousness, and the wide QRS indicates the ventricular contraction itself is less efficient than normal. IVR is often the rhythm you see in complete heart block, severe drug toxicity, or as a pre-arrest rhythm.
What Changed from Normal Sinus Rhythm
IVR changes everything from NSR: the pacemaker source (ventricles instead of SA node), the rate (20-40 instead of 60-100), the P waves (absent or dissociated), and the QRS (wide because the impulse travels through myocardium instead of the His-Purkinje system). The wide, slow, bizarre-looking QRS complexes are the hallmark.
Five Criteria: IVR vs NSR
- Rate: 20-40 BPM
- Profoundly bradycardic. This is the slowest inherent rate in the pacemaker hierarchy. Below 20 BPM, even the ventricular pacemaker is failing — asystole may be imminent.
- Regularity: Regular
- The ventricular pacemaker fires at a steady rate. RR intervals are consistent. The regularity at a slow rate with wide QRS is the signature pattern.
- P Waves: Absent or dissociated
- If the SA node is also dead, there are no P waves. If the SA node is still firing (as in complete heart block), P waves may be visible but march at their own rate, completely independent of the QRS complexes.
- PR Interval: Not applicable
- There is no relationship between atrial and ventricular activity. Even if P waves are visible, they bear no consistent timing relationship to the QRS complexes.
- QRS Complex: Wide (>0.12s)
- The impulse originates in the ventricular myocardium and does not use the normal His-Purkinje rapid conduction system. The QRS is wide (typically 0.14-0.16s), bizarre in morphology, and looks very different from the patient's normal QRS.
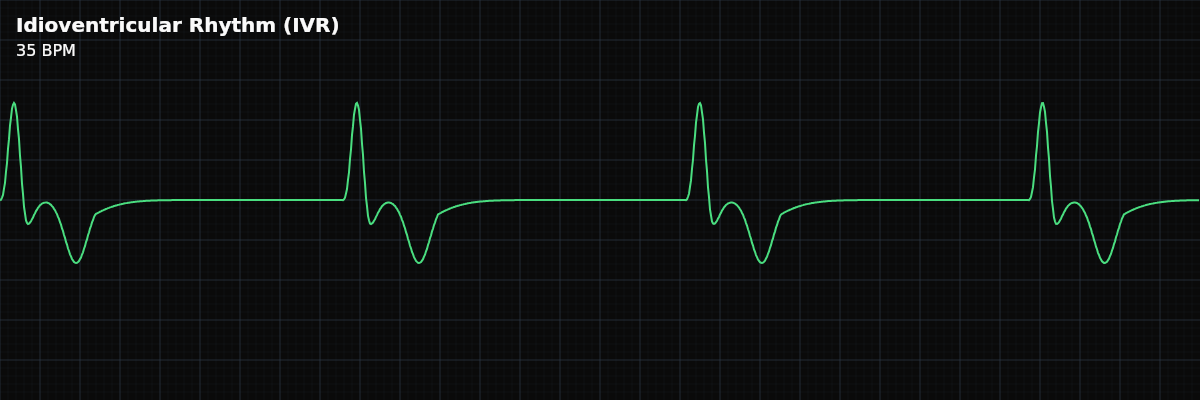
What IVR Looks Like on the Strip
On the strip, IVR is unmistakable: wide, slow, strange-looking QRS complexes at 20-40 BPM with no upright P waves preceding them. The complexes are wider and more bizarre than anything in normal sinus rhythm. The long gaps between complexes reflect the very slow rate. If you see independent P waves marching at their own faster rate, you are looking at complete heart block with IVR as the escape rhythm.
The Pacemaker Hierarchy
The heart has three backup levels, each slower than the last: **SA Node** — 60-100 BPM. Normal dominant pacemaker. Narrow QRS. **AV Junction** — 40-60 BPM. First backup when SA node fails. Narrow QRS (junctional escape). **Ventricles** — 20-40 BPM. Last backup when both SA node and junction fail. Wide QRS (idioventricular rhythm). IVR means you have reached the bottom of this hierarchy. There is no lower backup.
Clinical Context for Monitor Technicians
IVR most commonly occurs in complete (third-degree) heart block, where the AV node fails to conduct any impulses and the ventricles must generate their own rhythm. Other causes include severe sinus node dysfunction, drug toxicity (beta-blocker or calcium channel blocker overdose), severe hyperkalemia, and post-cardiac arrest as ventricular automaticity recovers.
When to Escalate
**Notify immediately:** - IVR at any rate — this indicates failure of all higher pacemakers - Patient is symptomatic — altered consciousness, hypotension, chest pain - Rate is dropping below 20 BPM — the ventricular escape is failing - No escape rhythm at all after a prolonged pause — approaching asystole IVR is never a "document and monitor" rhythm. It always requires prompt notification.
Putting It Together
Idioventricular rhythm is the heart's last-resort escape: wide QRS complexes at 20-40 BPM with absent or dissociated P waves. It means both the SA node and AV junction have failed. The ventricular pacemaker is the only thing keeping the heart beating. Never suppress IVR. Always notify the clinical team immediately.